
Case Report | DOI: https://doi.org/10.31579/2641-5194/035
Department of Pulmonary Medicine, T. N. Medical College, B. Y. L. Nair Hospital, Mumbai, India.
*Corresponding Author: Unnati Desai, Department of Pulmonary Medicine, T. N. Medical College, B. Y. L. Nair Hospital, Mumbai, India.
Citation: Vinod L. Pal, Dharani M, Utpat K., Desai U., Jyotsna M Joshi, Bharmal R. (2021) Pulmonary Thromboembolism and Pulmonary Fibrosis due to H1N1 Pneumonia with Acute Respiratory Distress Syndrome: Not ALL is COVID. J. Gastroenterology Pancreatology and Hepatobilary Disorders. 5(4): DOI: 10.31579/2641-5194/035
Copyright: © 2021, Unnati Desai, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 22 May 2021 | Accepted: 16 July 2021 | Published: 24 July 2021
Keywords: H1N1; ARDS; hypercoagulable state; venous thrombotic events; pulmonary thromboembolism(pte);
Novel influenza A H1N1 virus (pH1N1) was the predominant strain in the 2009 pandemic. It continues to circulate along with other influenza strains in the post pandemic era. This new virus is nevertheless well known for its strong association with high cardiovascular mortality and a high propensity to preferentially affect young and otherwise healthy adults, resulting in a clustering of severe and even fatal cases in patients of the productive age group. H1N1 infection is a multifaceted disease. It affects the lung parenchyma as well as the pulmonary vasculature. It also affects the multisystemic vasculature and can cause other embolic events not strictly falling in the “usual” thrombotic category. We herein present a case of H1N1 influenza pneumonia induced severe ARDS with pulmonary thromboembolism (PTE) and pulmonary fibrosis.
The novel influenza A (pH1N1 i.e. swine flu) virus illness, which is associated with high morbidity and mortality, is known to occur as pandemic as well as epidemic worldwide. The infection causes severe non cardiogenic hypoxemic respiratory failure also known as the acute respiratory distress syndrome (ARDS)[1,2]. In recent years, there has been an emergence of clinical data suggesting that pH1N1 infection may also predispose patients to the development of thromboembolic complications. Previous observational and autopsy studies have documented the occurrence of both venous and arterial events among patients with pH1N1 infection but the epidemiologic association between pH1N1 and thromboembolism as well as the pathophysiologic mechanisms underlying this potential association remains to be established. The prominence of pulmonary thromboembolism and infarction in this case may be related to hypercoagulability, which has also been reported elsewhere in patients with pandemic influenza pneumonia. Here we present a case of H1N1 influenza pneumonia induced severe ARDS with pulmonary thromboembolism (PTE). Our case also has concurrent post H1N1 pulmonary fibrosis described earlier in literature [3].
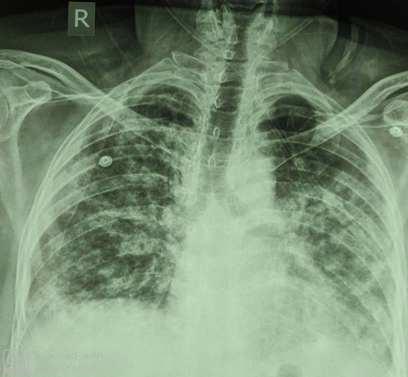
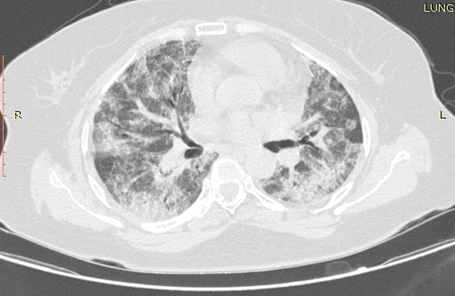
A 50 year old lady presented to the emergency medical services with complaints of sore throat, fever and dry cough since 1 week and progressive shortness of breath since 3 weeks. She was a housewife without any comorbidities and addictions. Patient had earlier followed up with private physician evaluated with throat swab for pH1N1 by reverse transcriptase polymerase chain reaction (RT PCR) method which was positive for pH1N1 infection. Patient was managed with broad spectrum antibiotics and oseltamivir 150mg twice daily for 2 weeks. Patient had no past history of tuberculosis, antituberculous drug intake or tuberculosis contact. There was a history of immobilization since 2 weeks. In view of chest radiograph (CXR) changes showing bilateral reticulonodular opacities with consolidation and persistent desaturation, she was referred to us for further management (figure 1). On examination the patient was afebrile with pulse of 111 beats per minute, blood pressure of 110/70 mmHg, respiratory rate of 28 cycles per minute and pulse oximetry showing saturation of 70% on room air, 90% with 1 litre/min of oxygen supplementation through nasal prongs. Respiratory system revealed bilateral basal crackles. Other system examination was unremarkable. Her complete hemogram (CBC) showed a hemoglobin of 13gm%, total count of 10500/cumm, platelets of 391000/cumm. Her renal and liver function tests were normal. Arterial blood gas (ABG) analysis was suggestive of type 1 respiratory failure with PaO2/FiO2 ratio of 200 indicating moderate ARDS. A repeat throat swab for pH1N1 RT-PCR was negative. A laboratory connective disease profile was negative. The Well score was 3 (moderate probability for PTE). Computed Tomography Pulmonary Angiography (CTPA) with high resolution computed tomography (HRCT) was suggestive of resolving bilateral diffuse ill defined bronchocentric and subpleural areas of consolidation, ground glass attenuation and patchy pulmonary fibrosis throughout the lung parenchyma with lower lobe predominance consistent with resolving ARDS with pulmonary fibrosis. Bilateral acute PTE with moderate thrombus burden was evident (figure 2a,3a). A two dimensional echocardiography (2D ECHO) as suggestive of mild pulmonary hypertension (PH) with pulmonary artery systolic pressure of 35 mm. In view of PTE she was started on anticoagulation with injectable low
molecular weight heparin (LMWH) and tablet warfarin. Patient was given oxygen supplementation with FiO2 60% then gradually FiO2 requirement decreased to 40%. She was also treated with oral steroids tablet prednisolone 40 mg once daily for 1 month followed by tapering dose (5 mg per week) for 6 months. After discharge from hospital patient was using oxygen supplementation at FiO2 of 28% which gradually decreased. At her one month follow up she was symptomatically much better with normal SpO2 on room air with a significant radiological improvement too. The repeat CTPA with HRCT was suggestive of residual pulmonary fibrosis with significant improvement in thrombus burden after 3 month of therapy with anticoagulants and steroids (figure 2b, 3b).
Hence we diagnosed this as a case of Pulmonary Fibrosis and Pulmonary Thromboembolism due to H1N1 pneumonia with ARDS.



ARDS is an entity characterized by acute onset respiratory symptoms with a non cardiogenic pulmonary edema and hypoxemic respiratory failure. It can emanate from a heterogeneous gamut of causes. These include infectious like severe bacterial fungal and viral pneumonia, sepsis, shock, trauma, burns and transfusion related insult. Influenza H1N1 infection can precipitate severe ARDS with very a high mortality [4]. Majority of patient of ARDS due to H1N1 had bilateral patchy opacity on computed tomography scan [6]. It is notorious for stimulating intravascular coagulation and its associated complications. The pathophysiology of thrombosis is based on the presence of three factors: Endothelial injury, venous status and hypercoagulability also termed as the Virchows triad. Damage to vascular walls prevents endothelium from inhibiting coagulation and initiating local fibrinolysis. Inflammatory response also plays a role in the formation of thrombus via production of microparticles (MPs) that carry cell-specific molecular proteins such as galectin [7]. The stimulation of monocytes, especially by galectin, leads to cell activation and tissue factor expression which triggers the coagulation pathway. Furthermore during inflammation, oxygen free radicals are produced which induce thrombosis in microvessels via activation of platelet aggregation [8]. Infectious agents, including viruses, bacteria and parasites, may initiate this process. An in vitro study reported that endothelial and monocytes cells that were incubated with influenza were able to activate coagulation via endothelial dysfunction and elevated tissue factor levels. Immobilization leads to local venous stasis by accumulation of clotting factors and fibrin, resulting in thrombi/emboli formation. In the Prospective Investigation of Pulmonary Embolism Diagnosis II (PIOPED II) study, immobilization was identified as the most common risk factor. The prophylactic administration of LMWH or unfractionated heparin in severely ill subjects is thereby recommended encouraged. The benefits of anticoagulation are weighed against the risks.
Seasonal influenza viruses may cause severe pulmonary disease and pulmonary embolism. The possible association between acute respiratory tract infections caused by seasonal influenza virus and the occurrence of PTE remains unknown till date. Mortality associated with pandemic influenza A was mostly due to respiratory conditions (76%). The direct cause of death was recorded as pulmonary embolism in only in 1% of these cases. However, in a study conducted in United States; of the hospitalized patients with H1N1 influenza A infection, 66% had pulmonary infiltrates suggestive of pneumonia or ARDS. Another study showed that the most common findings on CXRs were patchy consolidation but CXRs were normal in more than half of patients with pandemic H1N1 virus [2]. In our case pulmonary embolism was detected by CTPA performed due to a moderate wells pretest probability score. Additionally the symptoms of dyspnea, tachycardia with history of immobilization for 2 weeks led us to suspecting a possibility of pulmonary embolism. Our patient had no other risk factors for pulmonary embolism that we identified. Thus immobilization along with H1N1 infection would have triggered the coagulation cascade activation leading to hypercoagulable state. Despite of progress in the management of ARDS mortality still remains high. Influenza can cause severe ARDS because of high virulence load, abberant immune response and extensive lung damage. H1N1 ARDS patients may have long term lung disabilities [5]. Pulmonary fibrosis, a known sequelae could be progressive or regressive [3]. Our patient also had regressive pulmonary fibrosis as a sequelae. We describe for the first time PTE and Pulmonary fibrosis in a case of treated H1N1 pneumonia with ARDS. The timely recognition of clinical signs of ARDS, early introduction of antiviral therapy and lung protective ventilation play crucial roles in management.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
